


1Department of Dermatology, 3Department of Occupational and Environmental Medicine, University of Copenhagen, Bispebjerg Hospital and 2Department of Bacteria, Parasites, and Fungi, Statens Serum Institute, Copenhagen, Denmark
Hand eczema is frequently colonized with Staphylococcus aureus. Some patients with hand eczema wear occlusive gloves regularly; however, the effect of this on the density of S. aureus is unexplored. The aim of this study is to examine the effect of occlusive gloves on the density of S. aureus sampled from the hands of patients with hand eczema. In an experimental set-up, patients with moderate-to-severe hand eczema wore an occlusive glove on one hand for 4 h with a 30-min break. Bacterial swabs were collected from the most severe eczema lesion on the hand before and immediately after glove exposure. S. aureus colony-forming units were counted and log-transformations used for comparison of before- and after-values. Among 30 patients, 19 (63%) were colonized with S. aureus. After glove occlusion S. aureus colony-forming units increased by a factor of 1.72 (p < 0.01). In conclusion, the density of sampled S. aureus on eczematous skin after prolonged wearing of occlusive gloves is greatly increased.
Key words: hand eczema; Staphylococcus aureus; occlusive gloves; bacteria; alcohol-based hand rub; infection prevention.
Accepted Jul 1, 2021; Epub ahead of print Jul 5, 2021
Acta Derm Venereol 2021; 101: adv00515.
doi: 10.2340/00015555-3866
Corr: Line Brok Nørreslet, Department of Dermatology, University of Copenhagen, Bispebjerg Hospital, Bispebjerg Bakke 23, DK-2400 Copenhagen NV, Denmark. E-mail: line.brok.noerreslet.01@regionh.dk
Hand eczema is a common disease, particularly in professions such as healthcare, cleaning and catering, in which wearing occlusive gloves is often required. Recent findings show that more than 50% of all patients with hand eczema are colonized with the potentially harmful bacteria Staphylococcus aureus. This study explored how wearing occlusive gloves influenced Staphylococcus aureus colonization in patients with hand eczema. There was a major increase in the density of Staphylococcus aureus following occlusive glove wear, which probably negatively influences the prognosis of hand eczema, and is important regarding transmission of bacteria to the local environment.
Hand eczema (HE) is a common skin disease with a 1-year prevalence of nearly 10% in the general population of the Nordic countries (1), which is often caused or aggravated by occupational exposure, such as wet work. To date, little attention has been paid to the fact that more than 50% of all cases of HE are colonized with Staphylococcus aureus (2–4). Recently, this has been flagged up as possibly playing a part in the chronic course of the disease (5) and may furthermore pose a risk of contamination of the surrounding local environment.
Wearing occlusive gloves is an integral part of occupations associated with a high prevalence of HE, such as the healthcare sector and the food and cleaning industries (6–8), where occlusive gloves are used to protect the skin barrier from wet environments and trauma, and protect against becoming exposed to or transmitting pathogenic microorganisms. However, occlusive gloves generate heat and moisture inside the glove, and may consequently cause irritant contact dermatitis (9, 10). Theoretically, occlusive gloves may serve as a rich reservoir for bacteria to multiply (11, 12). The influence of prolonged wearing of occlusive gloves on bacterial growth on the hands has been only sparsely investigated (11–13). These studies found bacterial growth of commensal skin flora on non-eczematous hands of surgeons after an operation despite a pre-operational procedure including alcohol-based hand rub (ABHR) (11, 13).
Regarding ABHR, its immediate effectiveness in removing pathogenic bacteria, including S. aureus, from contaminated, healthy hands has been well documented (14, 15), whereas its effect on patients with HE is unknown. Patients with HE might be less compliant users of ABHR due to stinging and pain related to application of alcohol, and the effectiveness might be reduced if the ABHR does not reach S. aureus in the fissures or the scaly skin of HE.
The primary aim of this study was to determine the effect of occlusive gloves on the relative density of S. aureus sampled from the hands of patients with HE. Secondly, the study aimed to explore the effectiveness of once-applied ABHR on the density of S. aureus.
Patient population
Patients with chronic HE, as defined by the European Society of Contact Dermatitis (16), were recruited from the outpatient clinic of the Department of Dermatology, Bispebjerg University Hospital, Copenhagen, Denmark, from September 2019 to October 2020. Inclusion criteria were age ≥ 18 years and a HE Severity Index (HECSI) (17) score of > 17, corresponding to moderate-to-very-severe HE (18). Exclusion criteria were pregnancy, breastfeeding, and use of systemic or topical antibiotics within 4 weeks prior to study participation. Patients were included regardless of other types of treatment, which were nevertheless registered. The dermatologist-diagnosed sub-type of HE (19) (either irritant contact dermatitis, allergic contact dermatitis, hyperkeratotic, acute recurrent vesicular, or atopic HE), as well as current or past medical history of atopic dermatitis (AD) (“Have you had childhood eczema” (20), or “Have you had atopic dermatitis diagnosed by a dermatologist”) were noted.
The study was approved by the local ethics committee (project number H-18049625) and the Danish Data Protection Agency (project number VD-2019-15). Written informed consent was obtained from each patient.
Study design and sampling of S. aureus
The study was designed as a clinical trial with S. aureus sampling before and after standardized exposures to occlusive glove wear and ABHR, respectively. Patients were instructed not to use ABHR on the day of study participation, whereas usual hand washing was allowed. In addition, the intervention was performed in the morning, i.e. before job exposures. With a generation time, i.e. the doubling time or cell division rate, of approximately 30 min under laboratory conditions for S. aureus (21), it was hypothesized that exposure to occlusive glove wear for 2 h twice in one day would significantly increase the number of S. aureus in patients with HE. To mimic the everyday life of patients with HE working in different occupations where occlusive gloves are used repeatedly, the occlusive glove intervention was replicated after a break of 30 min. Therefore, the intervention with gloves was designed as follows: Non-bactericidal, powder-free, occlusive gloves were used on the hand hosting the most severe eczema for 2 h, followed by 30 min without a glove and subsequently another 2 h with a second, identical occlusive glove. Vinyl gloves (VWR, Leuven, Belgium) were chosen to protect the patients from potential sensitization to natural rubber latex or rubber chemicals. During the 30 min in between glove wear, the patients were not allowed to touch anything with the hand involved, in order to reduce potential bias from contamination. Before and immediately after the 4.5-h intervention period, the most severe eczematous lesion of the hand and a non-eczematous area on the back of the hand, each corresponding to an area of approximately 2 cm2, were sampled by rubbing the skin for 30 s using an ESwab (Copan, Brescia, Italy).
Five minutes after the end of the glove intervention, a sub-group of the patients was asked to rub their hands with 4 mL ABHR (cleansed water, 1.3% glycerol, 5% isopropyl alcohol and 85% ethanol by Amgros I/S), and another 5 min later new samples for S. aureus were collected from the 2 exact same locations as the prior sampling. The sub-group comprised the last 17 patients included in the study. The same investigator performed all sample and data collections.
Culturing and quantification of S. aureus
Swab samples were diluted in ultrapure phosphate-buffered saline (PBS). Then, 50 µl of undiluted and serial dilutions (×10 and ×100) of the transportation medium from the swab samples were plated in duplicates on S. aureus selective plates (SaSelect™, Bio-Rad, Marnes-la-coquette, France) and incubated for 20–24 h at 37°C. Colony-forming units (CFU) of S. aureus, identified by the pink colony colours on the selective plates, were counted on each plate by ocular inspection by experienced laboratory technicians. If more than 200 colonies were counted the sample was diluted 10-fold and plated again. The mean CFU was calculated based on the duplicates of each sample, and results from diluted samples were multiplied to assess the absolute CFU undiluted in the sample.
Statistical analysis
All values of CFU were log-transformed in order to obtain normality before comparisons and calculations. Comparison of CFU before and after occlusive glove wear and ABHR, respectively, was assessed using paired t-test of “before” and “after” log10-transformed values. A linear model was used to test for association between CFU (log10-transformed “before” sample) and HECSI. p-values <0.05 were considered statistically significant. R version 3.5.2 and RStudio were used (R Foundation for Statistical Computing, Vienna, Austria).
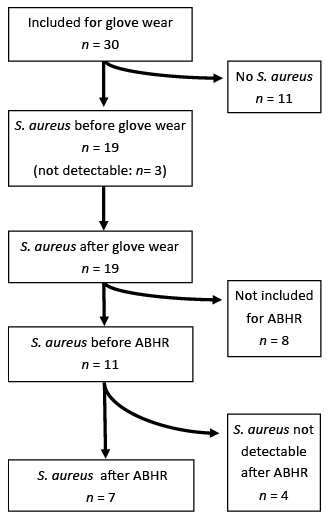
A total of 30 patients with chronic HE were included in the study and completed the glove intervention, and a sub-sample of patients (n = 17; 57%) also participated in the subsequent ABHR intervention (Fig. 1). Baseline demographics are shown in Table I. The mean ± standard deviation (SD) age of the study population was 49.5 ± 13.0 years, and 20 (66%) were females. A medical history of AD was reported in 11 patients (37%). The most prevalent HE sub-type was irritant contact dermatitis (n = 11; 37%) and atopic HE (n = 9; 30%), followed by allergic contact dermatitis (n = 5; 17%), hyperkeratotic (n = 3; 10%) and acute recurrent vesicular (n = 2; 7%) HE. Treatment comprised topical corticosteroids (n = 13; 43%), topical tacrolimus 0.1% (n = 2; 7%), and systemic therapy with methotrexate (n = 2; 7%) and alitretinoin (n = 1; 3%).
Fig. 1. Flow chart of the number (n) of patients with hand eczema with and without Staphylococcus aureus colonization on lesional skin included for occlusive glove wear and, subsequently, alcohol-based hand-rub (ABHR). Three patients were culture-negative before glove wear, but culture-positive after glove wear; thus they were also considered culture-positive before glove wear, although below the lower limit of detection. The last 17 patients included for glove wear also participated in the use of ABHR, of which 11 patients were colonized with S. aureus on lesional skin of hands and 6 patients were not colonized.
Table I. Baseline demographics and clinical data
The mean ± SD HECSI score for all patients was 66.1 ± 29.8 (Table I); and was higher in patients with S. aureus colonization on lesional skin (77.6 ± 34.0) compared with patients without S. aureus colonization (53.0 ± 17.3) (p = 0.02).
Occlusive glove wear
Prior to the glove intervention, 16 patients (53%) were colonized with S. aureus on lesional skin on the hands, and 11 patients (37%) were colonized on non-lesional skin. All patients colonized with S. aureus on non-lesional skin on the hands were also colonized on lesional skin. After occlusive glove wear, the relative S. aureus CFU count was increased, with a log10 (after/before)-ratio of 1.720 on lesional skin (p < 0.01), whereas no increase was observed for non-lesional skin (p = 0.63) (Table II). For 3 patients, S. aureus was identified after the intervention only, and since it is likely that S. aureus was present before the intervention, though below the detection limit in these patients, they are included in the calculation with “before” values of 1 CFU as stand-in for zero and below the lower limit of detection (Table II).
Table II. Staphylococcus aureus counts on lesional skin (LS) and non-lesional skin (NLS) of patients with hand eczema (n = 30) before and after occlusive glove wear for 2 + 2 hours and alcohol-based hand-rub
Lesional skin sample sites and the relative changes (log10-ratio) in S. aureus density following the glove intervention are shown in Fig. 2. Lesional skin samples were collected from the ventral side of the hand (n = 18) and the dorsal side of the hand (n = 12). The relative increase in S. aureus density after the glove intervention was similar on both sides of the hand.
Fig. 2. Sampling sites of the most severe lesion on the hands of patients with hand eczema. Positive (brown and red) and negative (blue) Staphylococcus aureus sampling sites. Size of circle illustrates the density of S. aureus fold change from before to after occlusive glove wear.
The relative increase (log10-ratio) in S. aureus density following occlusive glove wear was not related to HECSI score (p = 0.66).
The absolute S. aureus CFU/sample before wearing gloves for patients with S. aureus colonisation was not significantly correlated with increased HECSI (p = 0.17).
Alcohol-based hand-rub
Among the 17 patients participating in the use of ABHR after occlusive glove wear, 11 patients (65%) were colonized with S. aureus on lesional skin and of these, 4 patients (24%) were also colonized on non-lesional skin (Table II). A medical history of AD was reported in 8 (47%) of these patients. After the use of ABHR, S. aureus was detectable in 7 patients (mean HECSI=88), i.e. ABHR eradicated S. aureus in 4 patients (mean HECSI=63). The relative S. aureus CFU count on lesional skin decreased, with a log10 (after/before)-ratio of 2.516 (p < 0.01).
Knowing that 50–70% of patients with HE with moderate-to-severe disease are colonized by S. aureus on the hands, it is important to understand how commonly recommended procedures, such as the use of occlusive gloves and ABHR, affect S. aureus colonization. We found that the relative density of S. aureus increased dramatically on eczematous skin after the glove intervention. A single application of ABHR immediately after wearing occlusive gloves reduced the density of S. aureus from the eczematous lesions on the hands, but eradicated colonization in only less than half of the patients, which may have severe implications, e.g. for healthcare workers regarding transmission of bacteria to patients. These effects of commonly used and recommended procedures have, to our knowledge, not previously been investigated in patients with HE.
The mechanisms driving the large increase in density of S. aureus after occlusive glove wear in our patients are not fully understood. However, wet hands, in contrast to dry hands, have been documented to increase the likelihood of microbial transmission (22). Thus, factors such as heating and hyper-hydration of the skin surface underneath the glove may lead to higher S. aureus growth rate or to S. aureus being released from the surface and thereby being more accessible to a swab. We believe that both factors may explain the current results. Accordingly, this might also partly explain why we only observed a significant increase on the eczematous lesional skin with impaired skin barrier and not on the intact, non-lesional skin. S. aureus is a facultative anaerobic bacterium with a strain-specific growth rate that increases with higher temperatures (23). Patients were enrolled consecutively throughout 1 year, and consequently, the temperature and humidity of the examination room changed slightly. Generation times of S. aureus have been reported to range from 1 to 3 h during human nasal colonization (24). Therefore, cell division of S. aureus cannot solely explain our observed many-fold increase after 4.5 h. Acidic skin surface pH has been suggested to inhibit bacterial growth, dispersal and adhesion compared with more alkaline pH (25). In a previous study (26) skin pH increased after 4 days of occlusion of the arm of healthy volunteers, with an additional considerable increase in coagulase-negative staphylococci count, indicating that occlusion may cause the skin pH to become more alkaline and thereby contribute to bacterial growth, as observed in the current study. Adhesion, or binding capacity, of S. aureus to the skin may also be determined by other factors, such as lectin or sugar (glycocalyx) binding interactions (27). Likewise, S. aureus expresses a variety of adhesive surface proteins, so-called “microbial surface components recognizing adhesive matrix molecules” (MSCRAMMs), which bind more easily to atopic eczematous lesions than to intact skin (28). Whether these binding interactions are altered following glove wear needs to be explored. Other, unidentified mechanisms might contribute to explain the current results.
Occlusive glove wear is an integral part of wet work occupations, where HE is reported with a prevalence of up to 20% or even higher (6, 29). Several patients experience a chronic course of HE despite circumvention of relevant allergens and irritants. The potential role of S. aureus in the chronic aspect of HE has been suggested (5), and might be supported by the current results on the increased density of S. aureus following glove occlusion. The severity of HE in the patients in the current study was strongly related to the presence of S. aureus, supporting previous studies (2–4, 30, 31). The severity was not significantly associated with the density of S. aureus, in contrast to 2 previous studies (3, 30).
The impact of occlusive glove wear on S. aureus colonization also needs to be considered with respect to the risk of contamination of the local environment, particularly in the healthcare sector and the food industry. According to the Danish infection control and prevention recommendations in hospital settings (32), healthcare workers with HE should avoid close contact with patients and instead perform other tasks. The World Health Organization (WHO) states that occlusive gloves should be worn to prevent transmission of pathogenic microorganisms (33), especially when eczema is present (34). Therefore, a potential paradox is present: occlusive gloves are considered to protect from transmission of pathogenic bacteria, although they may serve as an “incubator” or reservoir for S. aureus, thus causing an even higher density of S. aureus once the gloves are removed or in case of puncture (11, 35), and eradication with ABHR may even be difficult.
Although ABHR is generally the first choice for hand hygiene in healthcare sectors (36) and is advised prior to glove wear in some procedures (33), its effectiveness varies and depends on compliance (37), the type of alcohol used (38), the application technique (39), the amount of ABHR used, and density of bacterial loads (38). We hypothesize, that the effectiveness of ABHR in patients with HE might be decreased due to high loads of S. aureus, increased adherence of S. aureus to the eczematous lesions, or due to insufficient rub of the painful ABHR application. Although the current results show that ABHR significantly reduced the density of S. aureus in patients with HE, complete eradication was observed in only a few patients.
Reduced time of exposure to occlusive gloves, or wearing cotton gloves underneath the occlusive gloves, could have influenced the current results of the glove intervention, making them less pronounced. Furthermore, the increase in density of the sampled S. aureus might have been reduced if bactericidal and/or powdered gloves had been used. Vinyl occlusive gloves were used in order to avoid the possible danger of sensitization, although the fit and permeability are different compared with those of nitrile or latex gloves, and the results are not directly transferable. However, there is no evidence to show that the use of latex or nitrile gloves would have changed the results of the current study.
The accuracy of the swab sampling technique, in contrast to the previously described “glove juice” method, where PBS liquid from inside a glove is used to assess S. aureus CFU released from the entire hand surface (3, 40) is a matter of debate. However, swabs are suitable for the investigation of specified sites, i.e. lesional and non-lesional skin, respectively, and for subsequent sampling and thereby the current study design, in which the “glove juice” method is not suitable. In order to minimize variation biases, the same investigator performed all samplings in a standardized manner and one of the same two laboratory technicians evaluated both cultures from each patient. Regarding the ABHR-intervention, it was a drawback that only a sub-group participated, and these results should be considered as preliminary findings to be further investigated in larger studies.
The current results are surprisingly clear; however, the current findings are required to be repeated and assessed using additional different study designs. Research into the dose–response relationship between length of time of occlusive glove wear and S. aureus growth is needed.
Little attention has been paid to S. aureus colonization in patients with HE, although it has been proposed to influence disease severity and prognosis, and furthermore, may result in contamination of the local environment. This study found that prolonged wear of occlusive gloves results in a sizeable increase in the density of S. aureus sampled from patients with HE. The use of ABHR reduced the density of S. aureus, although S. aureus was not completely eradicated in several of the patients with HE.
The authors thank Nrs Jette Holt, PhD, and Dr Anne Kjerulf, PhD, from the Department of Infectious Disease Epidemiology and Prevention at Statens Serum Institute, Copenhagen, Denmark, for valuable discussions about the study.
This work was supported by The Danish Working Environment Fund (grant number 20185100823); Augustinusfonden; and Aage Bangs Fond. The funding sources were not involved in this study, including the study design; the collection, analysis and interpretation of data; the writing of the paper; or the submission process.
Conflicts of interest: TA: Personal fees from advisory boards (Leo Pharma, Sanofi, Pfizer and Eli-Lilly); involved in Clinical trial (Abbvie); personal fees from consultancy, lectures (Leo Pharma, Sanofi); outside this paper. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize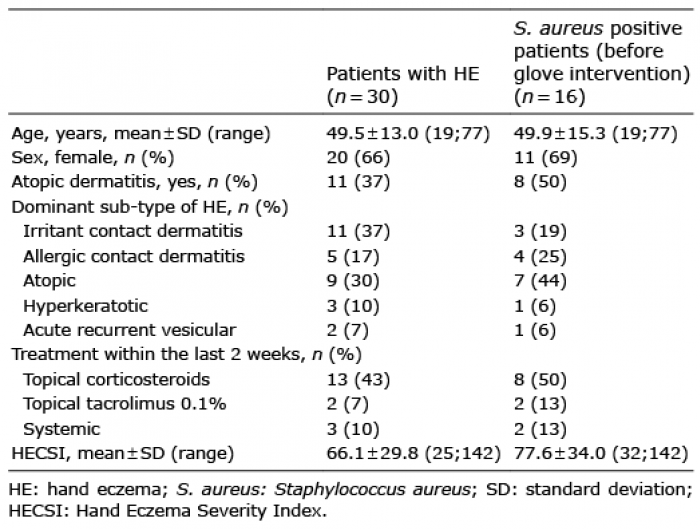 Click to show fullsize
Click to show fullsize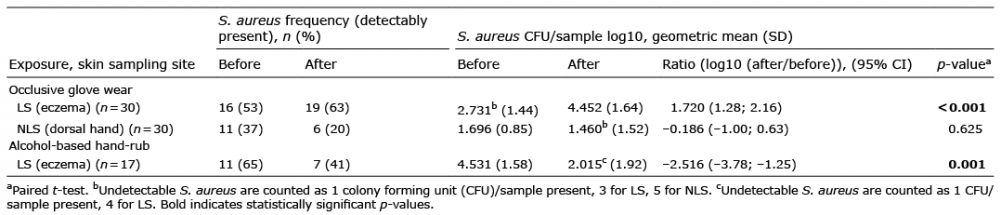 Click to show fullsize
Click to show fullsize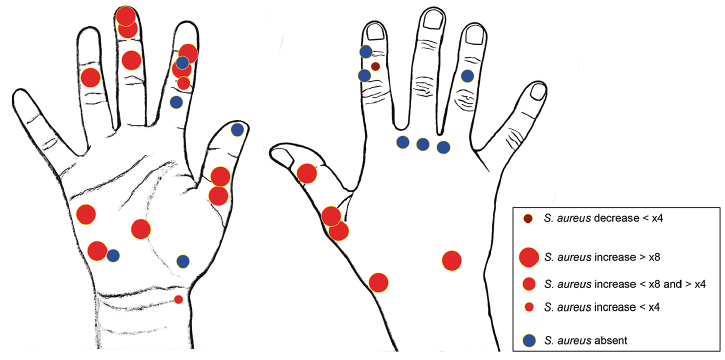 Click to show fullsize
Click to show fullsize